Vestibular, Balance, Vertigo, Tinnitus & Dizziness Rehabilitation in Victoria
 What is the Vestibular System?
What is the Vestibular System?
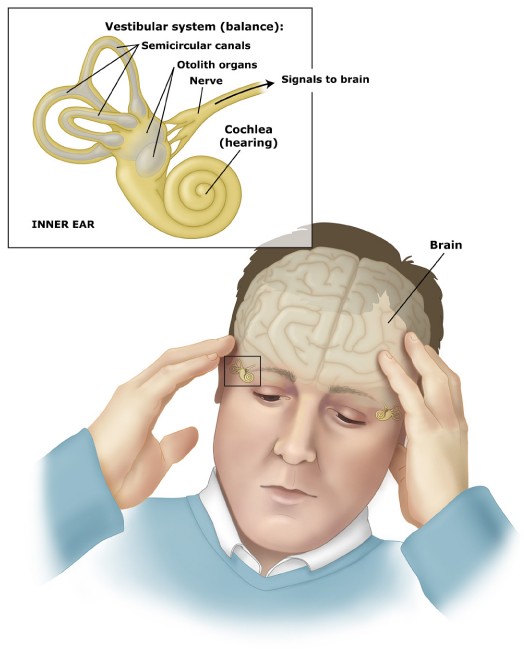
The vestibular system includes the parts of the inner ear (the organs of balance), the pathways that lead to the brain, and the brain itself that help control balance and eye movements. If the system is damaged by disease, aging, or injury, vestibular disorders or balance difficulties can result.
What are symptoms of a Vestibular problem?
The numbers of symptoms associated with vestibular dysfunctions are as varied as the number of causes. Some of the typical symptoms include:
- dizziness
- vertigo
- lightheadedness and disorientation
- poor balance
- headaches
- a spinning sensation
- difficulty reading or concentrating
- motion sensitivity
- difficulty concentrating
- poor tolerance of crowds
- blurry vision
- nausea and vomiting
- sensitivity to light
- fluctuating hearing
 What is Vestibular Rehabilitation?
What is Vestibular Rehabilitation?
Vestibular Rehabilitation Therapy (VRT) is an exercise-based program designed to promote central nervous system re-training for inner ear deficits. VRT can help with a variety of vestibular problems, including:
- Benign Paroxysmal Positional Vertigo (BPPV)
- Unilateral or bilateral vestibular hypofunction (reduced inner ear function on one or both sides)
- Ménière’s disease
- Labyrinthitis
- Vestibular neuritis
The primary goal with VRT is to retrain the brain to coordinate information from the inner ear balance organs, vision and the proprioceptive system (sensory receptors that are sensitive to stretch or pressure).
VRT is grounded in evidence-based medicine and has been extensively researched.
What will my first visit to VOR for Vestibular Rehabilitation involve?
One of our qualified Victoria Physiotherapists such as Jennifer Kolot and Rosie Chamberlin will perform a thorough evaluation that begins with a medical history to have you relate the severity & frequency of your symptoms, your triggers, and the impact your symptoms have on your life. The assessment includes evaluating your balance and gait, motion sensitivity, severity of vertigo, and the musculoskeletal system involved, to determine the source of the dizziness or balance problem.
What can I expect on subsequent visits?
All of our treatments are one-on-one with a qualified Physiotherapist and are up to 45 mins in duration. Treatments may include manual therapy on the vestibular balance organs or the neck, education about the balance system, and instruction on safe exercises appropriate for YOU and your recovery from a vestibular concern. All of our treatments are INDIVIDUALIZED and are tailored to YOUR NEEDS.
Victoria BC Vestibular Therapists

- Registered Physiotherapist
- Vestibular Physiotherapist
- Functional Dry Needling/IMS Certified
- ICBC Approved Physiotherapy Provider
- WorksafeBC Physiotherapy Provider
- Kinesiologist
- Soft Tissue Active Release
- Independent Contractor

- Registered Physiotherapist
- FCAMPT Manual and Manipulative Therapist
- Certified Gunn IMS Practitioner
- Herdman Certified Vestibular Rehabilitation Therapist
- TMJ Physiotherapy
ICS IMPULSE

ICS IMPULSE GOGGLES
We are pleased to offer the newest and most effective technology available for balance diagnosis. ICS Impulse is the Powerful New Gold Standard in Vestibulo-ocular Reflex Assessment.
“ICS Impulse is revolutionizing vestibular testing and taking it to a whole new level,” said Dan McNulty, general manager of GN Otometrics. “It is the culmination of almost two decades of research — a true collaboration between academia and industry — and it has resulted in the development of an innovative assessment device that has finally realized the potential in head impulse testing. It’s a major step forward for the industry and Otometrics is extremely proud to have been the driver in bringing this exceptional new device to market.”
Vestibulo-ocular Reflex Assessment Based on Real-life Stimuli, Plus Testing of All Six Canals
ICS Impulse generates objective measurement of both head and eye movement using a fast and precise system to assess the vestibulo-ocular reflex. The high-frequency stimuli used in vHIT is similar to that used in daily life, as when crossing a street, sitting in a restaurant or turning quickly toward a sound. ICS Impulse also features LARP/RALP functionality, which tests the anterior and posterior canals, enabling the assessment of all six semicircular canals, in a clinical setting — another industry first.
Unprecedented Testing Speed and Lightweight Goggles Enhance Patient Comfort
ICS Impulse revolutionizes the testing process, reducing overall testing time and enhancing patient comfort. A dramatically shorter testing time of 10 minutes, from patient entry to reporting, is rapidly establishing ICS Impulse as the first-line test conducted in vestibular assessment. Additionally, patient comfort is significantly improved by the ICS Impulse goggles, which are the lightest in the industry. They allow for smaller amplitude head impulses of only 15 to 20 degrees, which result in a more pleasant testing experience for the patient. Additionally, ICS Impulse enables the testing of children, bed-ridden patients or any patient for whom caloric testing is not an option.
“Our customers are often saying they don’t know how they assessed patients without this vital information,” said Wendy Crumley-Welsh, product manager ICS Impulse at GN Otometrics. “With ICS Impulse in their test battery, physicians around the world are realizing significant time-savings and have more confidence in their diagnosis of dizzy patients. Patient-friendliness, diagnostic accuracy of all six semicircular canals and time-efficiency are establishing ICS Impulse as the first test in our customers’ workflow.”
Extensive User Support
Otometrics has launched two dedicated Web sites to provide users with comprehensive support. At http://www.icsimpulse.com/, users will find extensive information and resources to learn more about ICS Impulse and vHIT. It features a library of educational materials including training videos, white papers and articles by experts which include instruction on how to conduct head impulse testing. There is also a blog where ICS Impulse users can communicate with the people behind the product, as well as other balance experts.
At http://www.headimpulse.com/, ICS Impulse users can explore both the science and practical application of head impulse testing. The online research library features research material, including videos of Dr. Halmagyi’s classroom lectures and examples of vHIT test results.
ICS Impulse will be featured in the Otometrics booth at several upcoming trade shows, conferences and meetings including: the Association of Research in Otolaryngology Mid-winter Meeting in February, where Curthoys is presenting; the American Academy of Neurology Annual Meeting, in March, where Halmagyi is presenting; the American Academy of Audiology AudiologyNow Conference in April and the American Academy of Otolaryngology-Head and Neck Surgery Annual Meeting in September.
ICS IMPULSE GOGGLES
Information from the Vestibular Disorders Association (VEDA)
ABOUT BALANCE, DIZZINESS, AND VESTIBULAR DISORDERS
The Human Balance System: A Complex Coordination of Central and Peripheral Systems
How the balance system uses sensory input from the eyes, muscles and joints, and inner ear to maintain balance and stable vision.
 Causes of Dizziness
Causes of Dizziness
Vertigo, dizziness, and disequilibrium are defined; common causes are explained.
Vestibular Disorders: An Overview
Describes the function of the vestibular system and symptoms and causes of damage to it; defines specific types of vestibular disorders; and reviews common diagnostic tests and treatments.
Vestibular Injury: Compensation, Decompensation, and Failure to Compensate
An explanation of how the balance system recovers from injury through the compensation process; acute (immediate) and chronic (long-term) compensation; causes of decompensation and failure to compensate; use of medication and vestibular rehabilitation therapy.
How Do I Know If I Have a Balance Disorder?
Describes the difference between dizziness, vertigo, and disequilibrium. Suggests questions a person might ask to help him or her decide whether to seek medical help for a balance problem or dizzy spell.
Possible Symptoms of a Vestibular Disorder
A quick reference for possible symptoms associated with inner ear balance disorders, including balance, vision, hearing, and cognitive issues.
DIAGNOSIS AND TREATMENT
Diagnostic Tests for Vestibular Problems
Descriptions and explanations of the purpose of various tests, including ENG (electro- videonystagmography), rotation tests, computerized dynamic posturography (CDP), audiometry, and scans (MRI, CT).
Trouble Getting a Diagnosis?
A list of reasons why many people with dizziness, imbalance, or vertigo have trouble obtaining a diagnosis, along with suggestions for speeding up the diagnostic process.
Vestibular Rehabilitation Therapy—An Effective, Evidence-Based Treatment
Describes the specialized form of exercise-based physical therapy designed to alleviate both primary and secondary symptoms of vestibular disorders. Includes descriptions of assessments of vision and eye movements, balance and gait, vertigo, and the musculoskeletal system; vestibular habituation, and balance retraining exercises. Dietary Considerations with Endolymphatic Hydrops, Ménière’s Disease, and Vestibular Migraine Dietary strategies for regulating inner-ear fluid balances; tips for reducing salt and sugar intake; examples of dietary migraine triggers, and a tip sheet for dining out.
Surgery for Peripheral Vestibular Disorders
Descriptions of surgical procedures used to repair or stabilize vestibular organs damaged by disease or injury. Procedures discussed include vestibular neurectomy, labyrinthectomy, transtympanic or intratympanic gentamicin treatment, endolymphatic sac decompression, oval or round window plugging, canal partitioning, PE tubes, and stapedectomy.
Common Misconceptions About ENG
Electronystagmography (ENG) has been the cornerstone of vestibular testing for more than fifty years. Yet there is some confusion about the extent and limitations of the information that can be obtained from an ENG examination. ENG refers to a battery of tests that examine specific aspects of the vestibular system. This battery consists of oculomotor tests, positioning and positional tests, and the caloric test. This document discusses these tests and their role in planning a vestibular rehabilitation program.
SPECIFIC VESTIBULAR DISORDER DIAGNOSES
Benign Paroxysmal Positional Vertigo (BPPV)
Discusses the cause of dizziness and vertigo symptoms resulting from positional changes, symptoms, causes, assessment, and treatment.
Vestibular Neuritis and Labyrinthitis: Infections of the Inner Ear
Viral versus bacterial infections of the inner ear; onset and symptoms; testing; treatment during the acute and chronic phases, including medication and vestibular rehabilitation exercises.
Ménière’s Disease
Describes the recurring set of symptoms resulting from abnormally large amounts of a fluid called endolymph collecting in the inner ear. Discussion includes symptoms, stages, diagnosis, treatment, and coping.
Balance and Aging
Good balance requires reliable sensory input from the individual’s vision, vestibular system and proprioceptors. With age, a variety of diseases can affect these systems. Discusses how a tendency to fall and have symptoms of dizziness should not be dismissed as unavoidable consequences of aging but may be important signs of a disease that might be cured or controlled.
Pediatric Vestibular Disorders
Vestibular disorders in children are generally considered uncommon. A vestibular system that is damaged by disease or injury in childhood can slow development of equilibrium and protective reflexes and motor-control tasks such as sitting unsupported, standing and walking.
Perilymph Fistula
A perilymph fistula is a tear or defect in one of the small, thin membranes that separate the middle ear from the fluid-filled inner ear. When a fistula is present, changes in middle ear pressure will directly affect the inner ear, stimulating the balance and/or hearing structures and causing symptoms.
Secondary Endolymphatic Hydrops
Describes symptoms of secondary endolymphatic hydrops, treatment with a diet regimen, and other quality of life issues.
Migraine-Associated Vertigo (MAV)
Migraine is now understood to be a vascular and neural process that can occur with or without pain. Migraine and vestibular dysfunction are discussed, including the recognition of migraine syndromes, evaluation and testing, vestibular test results commonly observed in migraine-related dizziness patients, treatment, and migraine triggers.
Ototoxicity
Discusses ototoxicity (ear poisoning) due to drugs or chemicals that damage the inner ear or vestibulo-cochlear nerve, which sends balance and hearing information from the inner ear to the brain.
Superior Canal Dehiscence: A Cause of Hearing and Balance Problems
Describes the vestibular and auditory symptoms and signs that can result from an opening (dehiscence) in the bone overlying the superior semicircular canal. Also discusses causes and diagnosis and treatment options.
Enlarged Vestibular Aqueduct Syndrome (EVAS)
Discusses the causes and prevalence of enlarged vestibular aqueduct syndrome (EVAS) and the hearing and vestibular symptoms associated with it, including information about clinical evaluation and treatment considerations.
VISION AND HEARING CHALLENGES WITH VESTIBULAR DISORDERS
Vision Challenges with Vestibular Disorders
Explains the link between the vestibular system and vision, describing the vestibulo-ocular reflex (VOR) in detail with information on evaluation, treatment, and coping strategies. Details the special considerations required for vision correction, including glasses and contact lenses.
Visual Preference and Vestibular Deficiency
A “Clinical Observations” column of VEDA’s member newsletter, “On the Level.” Discusses visual preference developed resulting from vestibular dysfunction, and provides suggestions for treating it.
Tinnitus—Ringing in the Ears: An Overview
Questions and answers about tinnitus, including terminology, causes and related factors, diagnosis and treatment options, and tips for prevention and reducing its severity.
Cochlear Hyperacusis and Vestibular Hyperacusis
Explains sound sensitivity, discusses symptoms that can include pain, dizziness, vertigo, imbalance, and others; causes; testing; and treatment options.
PSYCHOLOGICAL ASPECTS OF VESTIBULAR DISORDERS AND COPING STRATEGIES
Observations on Cognitive and Psychological Aspects of Vestibular Disorders
Includes comments from a social worker, an otolaryngologist, and a neuropsychologist during interviews by VEDA on how vestibular disorders affect cognitive and psychological or emotional functioning. Interviewees: Carolyn Bennett, ACSW; Alexander Schleuning II, MD; and Mark Tilson, PhD.
“It’s All in Your Head”: Addressing Vestibular Patients’ Stressors and Self Doubts
Identifies the issues associated with the subtle erosion of self-esteem often experienced by vestibular patients.
Coping with a Vestibular Disorder
This publication contains to articles: 1) “Coping with a Chronic Vestibular Disorder and Other Invisible Illnesses” by Molly-Jane Isaacson Rubinger, MSW, LICSW, and 2) Learning to Cope with Vestibular Disorders: Tips Offered by VEDA and support group leaders to the person who is new to vestibular disorders.
Fatigue, Stress and Responsibilities
This publication explains how one can learn to cope with the fatigue (and contributors to fatigue, including stress and pain) that often accompanies their chronic illness and offers strategies to manage stress.
OTHER
Vestibular Disease in Dogs and Cats
Explains the signs of vestibular dysfunction in pets. Includes causes, prognosis, and treatments, including what owners can do to help their pets. Also includes a picture and link to one beloved dog’s story.
VEDA Members Ask About Research
Addresses questions about why research takes so long, describes the scientific method, provides information about helping research by becoming a research subject.
Improving Balance with Tai Chi
Discusses the benefits of using Tai Chi – a martial art characterized by gracefully flowing movements and postures – to improve balance.
Hormones and Vestibular Disorders
Explores some of the possible effects of hormones on inner ear disorders in women.
GLOSSARY of DIZZINESS, BALANCE and VESTIBULAR TERMS
Acoustic neuroma – tumor of the vestibular nerve that may press on the hearing nerve causing dizziness and hearing loss.
Balance system – complex biological system that enables us to know where our body is in space and to keep the position we want. Proper balance depends on information from the labyrinth in the inner ear, from other senses such as sight and touch, and from muscle movement.
Benign positional vertigo – condition in which moving the head to one side or to a certain position brings on vertigo.
Brain Stem Auditory Evoked Response (BAER) – diagnostic test in which electrodes are attached to the surface of the scalp to determine the time it takes inner ear electrical responses. to sound to travel from the ear to the brain. The test helps locate the cause of some types of dizziness.
Caloric test – diagnostic test in which warm or cold water or air is put into the ear. If a person experiences certain eye movements (nystagmus) after this procedure, the labyrinth is working correctly.
Cholesteatoma – a tumorlike accumulation of dead cells in the middle ear. This growth is thought to result from repeated middle ear infections.
Computed Tomography (CT) Scan – radiological examination useful for examining the inside of the ear and head.
Diuretic – drug that promotes water loss from the body, through the urine. Used to treat hypertension, diuretics may bring on dizziness due to postural hypotension.
Dizziness – feeling of physical instability with regard the outside world.
Endolymph – fluid filling part of the labyrinth.
Hair cells – specialized nerves found in the semicircular canals and vestibule. Fibers (hairs) sticking out of one end of the hair cells move when the head moves and send information to the brain that is used to maintain balance.
Hyperventilation – repetitive deep breathing that reduces the carbon dioxide content of the blood and brings on dizziness. Anxiety may cause hyperventilation and dizziness.
Inner ear – contains the organs of hearing and balance.
Labyrinth – the organ of balance, which is located in the inner ear. The labyrinth consists of the three semicircular canals and the vestibule.
Meniere’s disease – condition that causes vertigo. The disease is believed to be caused by too much endolymph in the labyrinth. Persons with this illness also experience hearing problems and tinnitus.
Middle ear – the space immediately behind the eardrum. This part of the ear contains the three bones of hearing, the hammer (malleus), anvil (incus), and stirrup (stapes).
Multiple Sensory Deficits – condition associated with dizziness in which damage to nerves of the eye and arms or legs reduces information about balance to the brain.
Neurologist – physician who specializes in disorders of the nervous system.
Nystagmus – rapid back-and-forth movements of the eyes. These reflex movements may occur during the caloric test and are used in the diagnosis of balance problems.
Orthostatic hypotension – see postural hypotension.
Otologist – physician who specializes in diseases of the ear.
Peripheral vestibulopathy – vestibular disorder in which the vestibular nerve appears inflamed and paralyzed. Patients may have one or several attacks of vertigo.
Postural hypotension (also called orthostatic hypotension) – sudden dramatic drop in blood pressure when a person rises from a sitting, kneeling, or lying position. The prime symptom of postural hypotension, which is sometimes due to low blood volume, is dizziness or faintness. The condition can be dangerous in older persons, who may faint and injure themselves.
Semicircular canals – three curved hollow tubes in the inner ear that are part of the balance organ, the labyrinth. The canals are joined at their wide ends and are filled with endolymph.
Stroke – death of nerve cells due to a loss of blood flow in the brain. A stroke often results in permanent loss of some sensation or muscle activity.
Tinnitus – noises or ringing in the ear.
Transient Ischemic Attack (TIA) – temporary interruption of blood flow to a part of the brain. Because a TIA may signal the possibility of a stroke, it requires immediate medical attention. During a TIA, a person may feel dizzy, have double vision, or feel tingling in the hands.
Vertigo – severe form of dizziness in which one’s surroundings appear to be spinning uncontrollably. Extreme cases of vertigo may be accompanied by nausea.
Vestibular disorders – diseases of the inner ear that cause dizziness.
Vestibular nerve – nerve that carries messages about balance from the labyrinth in the inner ear to the brain.
Vestibular neuronitis – another name for peripheral vestibulopathy.
Vestibule – part of the labyrinth, located at the base of the semicircular canals. This structure contains the endolymph and patches of hair cells.
Vestibular Research Articles by Shelbourne Physiotherapist Peter Huijbregts
Dizziness in Orthopedic Physical Therapy Practice: Classification and Pathophysiology
Dizziness in Orthopedic Physical Practice: History and Physical Examination
Other Vestibular Rehabilitation Research Articles
Use of Virtual Reality Tools for Vestibular Disorders Rehabilitation: A Comprehensive Analysis
- Hall CD, Herdman SJ. Reliability of clinical measures used to assess patients with peripheral vestibular disorders.
J Neurol Phys Ther. 2006 Jun;30(2):74-81.
PMID: 16796772 [PubMed – indexed for MEDLINE] - Hall CD, Schubert MC, Herdman SJ. Prediction of fall risk reduction as measured by dynamic gait index in individuals with unilateral vestibular hypofunction.
Otol Neurotol. 2004 Sep;25(5):746-51.
PMID: 15354006 [PubMed – indexed for MEDLINE] - Schubert MC, Tusa RJ, Grine LE, Herdman SJ. Optimizing the sensitivity of the head thrust test for identifying vestibular hypofunction.
Phys Ther. 2004 Feb;84(2):151-8.
PMID: 14744205 [PubMed – indexed for MEDLINE] - Schubert MC, Das V, Tusa RJ, Herdman SJ. Cervico-ocular reflex in normal subjects and patients with unilateral vestibular hypofunction.
Otol Neurotol. 2004 Jan;25(1):65-71.
PMID: 14724495 [PubMed – indexed for MEDLINE] - Herdman SJ, Clendaniel RA. Re: Factors affecting recovery after acoustic neuroma resection by Cohen et al.
Acta Otolaryngol. 2003 Sep;123(7):889-90; author reply 891. No abstract available.
PMID: 14575408 [PubMed – indexed for MEDLINE] - Herdman SJ, Schubert MC, Das VE, Tusa RJ. Recovery of dynamic visual acuity in unilateral vestibular hypofunction.
Arch Otolaryngol Head Neck Surg. 2003 Aug;129(8):819-24.
PMID: 12925338 [PubMed – indexed for MEDLINE] - Schubert MC, Herdman SJ, Tusa RJ. Vertical dynamic visual acuity in normal subjects and patients with vestibular hypofunction.
Otol Neurotol. 2002 May;23(3):372-7.
PMID: 11981398 [PubMed – indexed for MEDLINE] - Schubert MC, Herdman SJ, Tusa RJ. Functional measure of gaze stability in patients with vestibular hypofunction.
Ann N Y Acad Sci. 2001 Oct;942:490-1. No abstract available.
PMID: 11710496 [PubMed – indexed for MEDLINE] - Herdman SJ, Schubert MC, Tusa RJ. Strategies for balance rehabilitation: fall risk and treatment.
Ann N Y Acad Sci. 2001 Oct;942:394-412. Review.
PMID: 11710480 [PubMed – indexed for MEDLINE] - Herdman SJ, Schubert MC, Tusa RJ. Role of central preprogramming in dynamic visual acuity with vestibular loss.
Arch Otolaryngol Head Neck Surg. 2001 Oct;127(10):1205-10.
PMID: 11587600 [PubMed – indexed for MEDLINE] - Herdman SJ, Blatt P, Schubert MC, Tusa RJ. Falls in patients with vestibular deficits.
Am J Otol. 2000 Nov;21(6):847-51.
PMID: 11078074 [PubMed – indexed for MEDLINE] - Blatt PJ, Georgakakis GA, Herdman SJ, Clendaniel RA, Tusa RJ. The effect of the canalith repositioning maneuver on resolving postural instability in patients with benign paroxysmal positional vertigo.
Am J Otol. 2000 May;21(3):356-63.
PMID: 10821549 [PubMed – indexed for MEDLINE] - Herdman SJ, Blatt PJ, Schubert MC. Vestibular rehabilitation of patients with vestibular hypofunction or with benign paroxysmal positional vertigo.
Curr Opin Neurol. 2000 Feb;13(1):39-43. Review.
PMID: 10719648 [PubMed – indexed for MEDLINE] - Yen MT, Herdman SJ, Tusa RJ. Oscillopsia and pseudonystagmus in kidney transplant patients.
Am J Ophthalmol. 1999 Dec;128(6):768-70.
PMID: 10612521 [PubMed – indexed for MEDLINE] - Suzuki AR, Herdman SJ, Tusa RJ. [Diagnosis and therapeutic options in benign paroxysmal positional vertigo]
Acta Otorrinolaringol Esp. 1999 Mar;50(2):106-17. Review. Spanish.
PMID: 10217683 [PubMed – indexed for MEDLINE] - Herdman SJ, Tusa RJ, Blatt P, Suzuki A, Venuto PJ, Roberts D. Computerized dynamic visual acuity test in the assessment of vestibular deficits.
Am J Otol. 1998 Nov;19(6):790-6.
PMID: 9831156 [PubMed – indexed for MEDLINE] - Herdman SJ. Role of vestibular adaptation in vestibular rehabilitation.
Otolaryngol Head Neck Surg. 1998 Jul;119(1):49-54. Review.
PMID: 9674514 [PubMed – indexed for MEDLINE] - Monsell EM, Furman JM, Herdman SJ, Konrad HR, Shepard NT. Computerized dynamic platform posturography.
Otolaryngol Head Neck Surg. 1997 Oct;117(4):394-8.
PMID: 9339802 [PubMed – indexed for MEDLINE] - Herdman SJ. Advances in the treatment of vestibular disorders.
Phys Ther. 1997 Jun;77(6):602-18. Review.
PMID: 9184686 [PubMed – indexed for MEDLINE] - Tusa RJ, Grant MP, Buettner UW, Herdman SJ, Zee DS. The contribution of the vertical semicircular canals to high-velocity horizontal vestibulo-ocular reflex (VOR) in normal subjects and patients with unilateral vestibular nerve section.
Acta Otolaryngol. 1996 Jul;116(4):507-12.
PMID: 8831834 [PubMed – indexed for MEDLINE] - Turano KA, Dagnelie G, Herdman SJ. Visual stabilization of posture in persons with central visual field loss.
Invest Ophthalmol Vis Sci. 1996 Jul;37(8):1483-91.
PMID: 8675390 [PubMed – indexed for MEDLINE] - Herdman SJ, Tusa RJ. Complications of the canalith repositioning procedure.
Arch Otolaryngol Head Neck Surg. 1996 Mar;122(3):281-6.
PMID: 8607956 [PubMed – indexed for MEDLINE] - Herdman SJ, Clendaniel RA, Mattox DE, Holliday MJ, Niparko JK. Vestibular adaptation exercises and recovery: acute stage after acoustic neuroma resection.
Otolaryngol Head Neck Surg. 1995 Jul;113(1):77-87.
PMID: 7603726 [PubMed – indexed for MEDLINE] - Turano K, Rubin GS, Herdman SJ, Chee E, Fried LP. Visual stabilization of posture in the elderly: fallers vs. nonfallers.
Optom Vis Sci. 1994 Dec;71(12):761-9.
PMID: 7898883 [PubMed – indexed for MEDLINE] - Herdman SJ. Canalith repositioning maneuver.
Otolaryngol Head Neck Surg. 1994 Nov;111(5):691; author reply 691-2. No abstract available.
PMID: 7848466 [PubMed – indexed for MEDLINE] - Hain TC, Herdman SJ, Holliday M, Mattox D, Zee DS, Byskosh AT. Localizing value of optokinetic afternystagmus.
Ann Otol Rhinol Laryngol. 1994 Oct;103(10):806-11.
PMID: 7944173 [PubMed – indexed for MEDLINE] - Herdman SJ, Sandusky AL, Hain TC, Zee DS, Tusa RJ. Characteristics of postural stability in patients with aminoglycoside toxicity.
J Vestib Res. 1994 Spring;4(1):71-80.
PMID: 8186864 [PubMed – indexed for MEDLINE] - Turano K, Herdman SJ, Dagnelie G. Visual stabilization of posture in retinitis pigmentosa and in artificially restricted visual fields.
Invest Ophthalmol Vis Sci. 1993 Sep;34(10):3004-10.
PMID: 8360031 [PubMed – indexed for MEDLINE] - Herdman SJ, Tusa RJ, Zee DS, Proctor LR, Mattox DE. Single treatment approaches to benign paroxysmal positional vertigo.
Arch Otolaryngol Head Neck Surg. 1993 Apr;119(4):450-4.
PMID: 8457308 [PubMed – indexed for MEDLINE] - Konrad HR, Tomlinson D, Stockwell CW, Norre M, Horak FB, Shepard NT, Herdman SJ. Rehabilitation therapy for patients with disequilibrium and balance disorders.
Otolaryngol Head Neck Surg. 1992 Jul;107(1):105-8. Review.
PMID: 1528589 [PubMed – indexed for MEDLINE] - Tian J, Herdman SJ, Zee DS, Folstein SE. Postural stability in patients with Huntington’s disease.
Neurology. 1992 Jun;42(6):1232-8.
PMID: 1534875 [PubMed – indexed for MEDLINE] - Tusa RJ, Repka MX, Smith CB, Herdman SJ. Early visual deprivation results in persistent strabismus and nystagmus in monkeys.
Invest Ophthalmol Vis Sci. 1991 Jan;32(1):134-41.
PMID: 1987095 [PubMed – indexed for MEDLINE] - Tian JR, Herdman SJ, Zee DS, Folstein SE. Postural control in Huntington’s disease (HD).
Acta Otolaryngol Suppl. 1991;481:333-6.
PMID: 1833947 [PubMed – indexed for MEDLINE] - Herdman SJ. Treatment of benign paroxysmal positional vertigo.
Phys Ther. 1990 Jun;70(6):381-8. Review.
PMID: 2189146 [PubMed – indexed for MEDLINE] - Herdman SJ. Exercise strategies for vestibular disorders.
Ear Nose Throat J. 1989 Dec;68(12):961-4.
PMID: 2620646 [PubMed – indexed for MEDLINE] - Tusa RJ, Demer JL, Herdman SJ. Cortical areas involved in OKN and VOR in cats: cortical lesions.
J Neurosci. 1989 Apr;9(4):1163-78.
PMID: 2703872 [PubMed – indexed for MEDLINE] - Herdman SJ, Tusa RJ, Smith CB. Cortical areas involved in horizontal OKN in cats: metabolic activity.
J Neurosci. 1989 Apr;9(4):1150-62.
PMID: 2703871 [PubMed – indexed for MEDLINE] - Zee DS, Tusa RJ, Herdman SJ, Butler PH, Gucer G. Effects of occipital lobectomy upon eye movements in primate.
J Neurophysiol. 1987 Oct;58(4):883-907.
PMID: 3681400 [PubMed – indexed for MEDLINE] - Tusa RJ, Zee DS, Herdman SJ. Effect of unilateral cerebral cortical lesions on ocular motor behavior in monkeys: saccades and quick phases.
J Neurophysiol. 1986 Dec;56(6):1590-625.
PMID: 3806184 [PubMed – indexed for MEDLINE] - Krebs DE, Harris SR, Herdman SJ, Michels E. Theory in physical therapy.
Phys Ther. 1986 May;66(5):661-2. No abstract available.
PMID: 3703928 [PubMed – indexed for MEDLINE] - Schank JA, Herdman SJ, Bloyer RG. Physical therapy in the multidisciplinary assessment and management of osteoarthritis.
Clin Ther. 1986;9 Suppl B:14-23.
PMID: 3829092 [PubMed – indexed for MEDLINE] - Herdman SJ, Hand CL, Hand PJ. Autoradiographic deoxyglucose study of visually activated extrastriate cortex in the primate: three-dimensional reconstruction.
Exp Neurol. 1984 Aug;85(2):383-90.
PMID: 6745380 [PubMed – indexed for MEDLINE] - Yu J, Chambers WW, Liu CN, Herdman SJ, Chen WP. Induction of spinal seizures by natural stimulation in cats.
Brain Res. 1984 May 14;299(2):323-30.
PMID: 6733453 [PubMed – indexed for MEDLINE] - Herdman SJ, Douglas MA, Shell DR, Volz DL, Yancey SD, Chambers WW, Liu CN. Recovery of the hopping response after complete spinal cord transection in the cat.
Exp Neurol. 1983 Sep;81(3):776-80.
PMID: 6884485 [PubMed – indexed for MEDLINE] - Herdman SJ. Effect of experience on recovery following CNS lesions.
Phys Ther. 1983 Jan;63(1):51-5. No abstract available.
PMID: 6849007 [PubMed – indexed for MEDLINE] - Herdman SJ. Recovery of shivering in spinal cats.
Exp Neurol. 1978 Apr;59(2):177-89. No abstract available.
PMID: 639914 [PubMed – indexed for MEDLINE]
Dizziness-What is it? Why does it happen? What can be done about it?
308-1175 Cook Street
Victoria,
British Columbia
V8V 4A1
CAPhone: 250-381-9828
Website: https://physiotherapyvictoria.ca